What is Center Mass? The generally accepted definition is “center of the chest.â€Â This is usually denoted on a target by an X score ring or similar point of aim to aid in training. Unfortunately, this is wrong insofar as reality is concerned (and we should always be concerned with reality). Center Mass is the center of the target offered or selected. It is a point of aim selected by the shooter based on preference or circumstance that provides the best margin of error for quality service under stress.Â
Since the term Center Mass is most often associated with the center of the chest, or the Thoracic Cavity, it has become the functional definition even though it is incorrect under many circumstances. Is this just semantics? I don’t think so. I personally consider it to be another firearms training meme that promotes memorization under ideal conditions and does not address the potential reality of a violent encounter. In order to be the most effective shooter, our reality of center mass should reflect what we are actually talking about and that is shooting people, not paper. The intent of shooting to incapacitate your threat as efficiently and quickly as possible; and that is best done with a firm understanding of the body and how best to defeat it as it is presented to you.
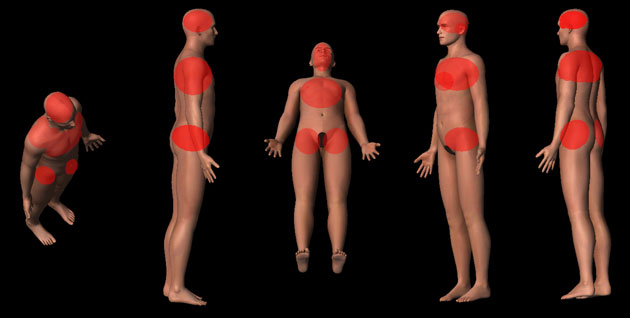
The human body, generally speaking, does not react well to gunfire. Bullets propelled at speed have very destructive characteristics that exceed the body’s ability to cope with trauma on a varied scale depending on where the bullet strikes and what it strikes. Nature also saw fit to clump the majority of critical organs together and because of this, coupled with the reasonable desire to aim for the area of the body with the highest margin of error, we get center mass shooting.
But just because it provides the highest margin of error, that does not mean it’s the most efficient or the ideal area to attempt to target across all possible situations. We sacrifice varying degrees of incapacitating ability by targeting the thoracic cavity over the head (specifically the cranial vault). This is taught because of the small size of the head when compared to the upper chest and because of a dependence on two-dimensional training models and targets built around the center mass preference. The fact is one of three things happen when the body is struck by a bullet:
- An immediate reaction
- A delayed reaction
- No reaction
Of the first two, you have a physiological and a psychological reaction.
A physiological reaction is when the bullet destroys critical organs, vessels, tissue, bone or nerve communications that causes a severe interruption or cessation in body functions necessary for a threat to continue to fight. This can be immediate (such as a strike to the cranial vault) or delayed (such as a strike to an artery, lung, liver or even heart). The damage caused by the bullet in this case requires no decision on the part of the threat to result in an effect on their performance.
A psychological incapacitation is where a threat, either due to injury or fear of one, ceases to fight and/or surrenders. This sort of incapacitation is not reliable because it cannot be predicted and should not be expected. Reliance on any action with the intention of causing a psychological incapacitation is dangerous.
There is no Off Switch in the chest.
The Center Mass thoracic cavity does not contain an off switch, medically speaking. Even considering the heart, the life-giving pump that pushes blood to all our organs, muscles and other bits and pieces; a direct hit to the heart with common small arms ammunition will not produce an instant incapacitation. Multiple hits to the heart and surrounding area are also highly unlikely to produce an instant incapacitation. Training to target the chest has never been about an off switch. It’s about a margin of error and a collection of critical organs needed for the threat to fight. The more damage inflicted on these organs, the quicker the threat will lose the ability to fight. This ability isn’t lost instantly. Organ failure, exsanguination (blood loss) takes time and the amount of time it takes cannot be reliably predicted across the board.
However, consider this.
For an average 175 pound male, the cardiac output will be 5.6 liters per minute. His blood volume will be 1.3 Gallons. Assuming his cardiac output can double under stress (as his heart beats faster with greater force), his aortic blood flow can reach 12-13 liters (2.6+ Gallons) per minute. Even if a wound totally severs the Thoracic Aorta, then it would take 4.7 seconds to lose 20% of his blood from one point of injury. The loss of 20% of blood is required for the body to fail, generally speaking; which causes the central nervous system to fail resulting in unconsciousness.
Wounds do not usually bleed at this rate because small arms ammunition (especially handgun rounds) do not always (completely) sever arteries when they strike them, undamaged tissue near the permanent wound cavity acts as a barrier to blood loss and as blood pressure falls, blood flow slows. Also, even a strike to the heart, which is a muscular organ, may not be as damaging as a strike to surrounding vessels such as the aorta or vena cava (Superior or Inferior) because unlike the heart, these vessels are thin walled and often tear when struck.

Does this mean we should discard the thoracic cavity as a point of aim if it’s available? Absolutely not. It just means we need to have realistic expectations on performance and be implicitly prepared for a threat to have the will and ability to fight even after suffering wounds to the center mass region.
“We shoot until the threat stops†is another popular firearms meme, and one I totally agree with. It means you literally stay on the gun until your threat has lost mobility and fighting ability, which means surrender or unconsciousness. You give them as many rounds as you can accurately shoot in the shortest amount of time possible so long as they give you a clear point of aim and a reason to shoot them.  Can a threat collapse to the ground and still fight? Of course; be prepared for it and train for it.
The lateral pelvis, this shit isn’t magic.
Targeting the pelvis to collapse a threats load bearing structure and ability to fight isn’t new. The pelvis has long been an ideal target to cause mobility damage since the days of swords, spears and warriors on horseback. The pelvis is where we generate our movement from. Though the number of critical organs in this area is zero and for critical vessels we have the femorals branching off from the aorta. Remember, we can only rely on a physiological incapacitation. A good strike to the lateral pelvis may turn a fleeing/moving felon into a stationary felon but it wont remove their ability to fire a weapon and its certainly unlikely to change their unfavorable opinion of you.
Lateral pelvis targeting has found a home in modern training and I agree with it so long as its taught and understood realistically. The lateral pelvis is an ideal point of aim if I cannot get the torso or the head; otherwise its third on my list of places to put bullets. There are some out there selling it like wolf tickets as a magical place to target where incapacitation is all but guaranteed. Immobilization is not incapacitation.
Center Mass in the Real World
In order for a threat to deliver accurate gunfire, they only need two things; and eye and an arm. A bad guy can totally conceal all but their weapon hand and one eye behind a piece of cover and shoot accurately.

Where is center mass? More importantly, have you practiced or been trained for this possibility so you recognize center mass? Of the possible “what if†scenarios, I would consider this the worst. Imagine confronting and armed and incredibly violent felon in a parking garage or street corner who tucks all but an extended weapon and the leading edge of their head behind a concrete pillar or the corner of a brick building. What options would you have?
A vital hit would require a strike to the head; with a target width of perhaps six inches, this would be a difficult shot under manufactured training stress, let alone the stresses of real life. Do you seek cover and hope they change position (if you had such a position, would you move)? Or, do you work with the reality of the three dimensional world and press to change your angle; attempt to flank your threat or, lacking cover of your own, press them quickly to overcome their decision making ability? Of course there is no easy answer.
Where is center mass on a threat engaging you from the ground?
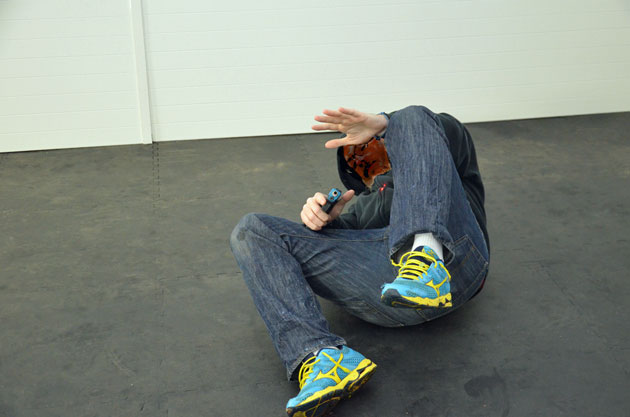
Where is it on a threat seated in a car or taking cover behind a car?

Where is center mass on a threat crawling through a window? If you have been trained and practice on ideal targets that are standing tall and squared to you, do you wonder if perhaps you are conditioning yourself to only shoot when the threat presents in this way? Do you think such practice could cause you to hesitate when a threat uses cover, attacks from an odd physical position or initiates a fight from cover?
I personally believe that training and practicing in this way can (and has) caused hesitation, which is something we do not what to instill in any training or practice involving the use of force. Waiting for a clear shot with a clear backdrop is one thing; waiting for a threat to present in a more ideal position even as they are trying to injure you can be harmful to your health to say the least.
The Magic Bullet Formula
Overheard in conversations, seen in online comments or spoken to me in person; I have seen or heard a large number of magic formulas for stopping a threat. Most of them are about the bullet or caliber. The .45, the .357, and even the .40 are blessed by some with magical powers, as if these rounds can expand to the size of pie plates or in some other way grossly outwit physiology (and physics) and/or common sense.
The fact is, handguns are poor manstoppers when compared to some rifles (and some rifles are poor man stoppers as well). Gunfights are won by shot placement and round penetration. As much as people love the venerable .45 ACP round, its expansion as an average hollow point round is around .08″ more than a 9mm and the 9mm consistently provides better penetration. The .40 S&W performs on par with the 9mm across a broad number of self-defense rounds, but there simply is no handgun round of a popular and practical caliber that provides the wound characteristics of a rifle round.
A wound with .10″ or even an inch greater diameter entrance will not provide a superior benefit that can be relied upon because each shooting is different and as already mentioned, outside of an immediate reaction to gunfire (a CNS failure) we have to rely on blood loss to cause incapacitation. Is a hollow point that expands (if it expands) .08″ more than a different round going to provide a significant advantage? Perhaps but I would say no because each shooting is unique and no matter how lauded a round’s performance is in testing, you can count on favorable examples being cherry picked and bad examples to be ignored by whoever wishes to favor whatever round.
Every round out there has failed at some point; either in testing on different materials or conditions or against a live threat. For those that failed against a live threat, it probably wasn’t because of the round but rather where the round struck the body.  Round placement and penetration. The more rounds I have per magazine, the more chances I have to stop a threat before I am forced to reload. I wouldn’t pick any round or caliber based on hyperbole or nostalgia any more than I would pick my brain surgeon.
And of course the other side of magic formulas;
“Ill just shoot him in the legs.â€
“Two to the chest, one to the head.â€
“Double tap and done.â€
“Ill just shoot him in the pelvis and work my way up.â€
All of these “plans†presuppose that your bad guy will let you. We shoot to stop the threat and doing so means targeting the center of what is offered, or exercising discipline until you can maneuver for a clear shot or wait for the threat to give you one. We should be wary of anything that always works on paper, just as we should probably be dubious of magic formulas that require a specific set of circumstances to work. The only off switch is a hit (or more) to the central nervous system. Outside of that, you can and should expect a threat to continue to fight regardless of where or how many times you hit them. Until they lose consciousness or surrender, they are still a threat and should be treated as such by the continued use of controlled violence so long as you have a clear shot.

Center mass, flank crouch

Center mass, rear presentation
When it’s time to practice for the use of force in three dimensions, consider the human body and how it may present to you; flank shots, shooting the bad guy in the back (yes, defense of a third party), shooting a threat that has been put on the ground, or is using cover; the possibilities are nearly endless. There are many good sources of realistic 3-D targets out there and no lack of information on anatomy, shooting, round performance and the body’s responses to stress.  Total preparation is about the gun as much as it is the mind and what knowledge you can bring to the fight.
Train accordingly.
Good read. Very informative
I agree, very good read
Really enjoyed this article. A ton of great information in here.
I am saving this article as a PDF and referring to it often.
This article shows some flaws in my thinking and my own training plans. I have often fired a mag or two into the center of mass but have also practiced head shots. That is with a pistol. I make my first shot when using a rifle to the head. Good guys aren’t the only ones using body armor nowdays and a 7.62×51 to the head is fight over. I broke my pelvis in an accident several years ago and the idea of a shot to the pelvis never occured to me until I read your article. Thanks for the great article.
Louis Awerbuck has a simple method to help train for this even on a square range. Overly simplified, staple your B-27ish target with a convex bow to it then place the target stand at various angles. Helps vizualize shooting “through” center mass, not for the “X-ring.”
mr cowan’s writing is very very well done, he is on my list of folks to take a class from…love reading his view points